

A robotic doctor that can be controlled hundreds of kilometres away by a human counterpart is gearing up for action.
Getting a check-up from a robot may sound like something from a sci-fi film, but scientists are closing in on this real-life scenario and have already tested a prototype.
“The robot at the remote site has different force, humidity and temperature sensors, all capturing information that a doctor would get when they are directly palpating (physically examining) a patient,” explains Professor Angelika Peer, a robotics researcher at the University of the West of England, UK.
Prof. Peer is also the project coordinator of the EU-funded ReMeDi project, which is developing the robotic doctor to allow medical professionals to examine patients over huge distances.
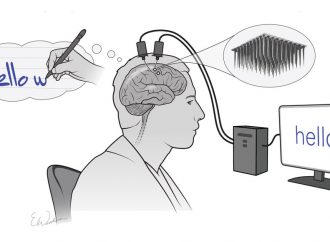
Through a specially designed surface mounted on a robotic arm, stiffness data of the patient’s abdomen is displayed to the human, allowing the doctor to feel what the remote robot feels. This is made possible thanks to a tool called a haptic device, which has a soft surface reminiscent of skin that can recreate the sense of touch through force and changing its shape.
During the examination, the doctor sits at a desk facing three screens, one showing the doctor’s hand on the faraway patient and a second for teleconferencing with the patient, which will remain an essential part of the exchange.
The third screen displays a special capability of the robot doctor – ultrasonography. This is a medical technique that sends sound pulses into a patient’s body to create a window into the patient. It reveals areas of different densities in the body and is often used to examine pregnant women.
Ultrasonography is also important for flagging injuries or disease in organs such as the heart, liver, kidneys or spleen and can find indications for some types of cancer, too.
“The system allows a doctor from a remote location to do a first assessment of a patient and make a decision about what should be done, whether to transfer them to hospital or undergo certain treatments,” said Prof. Peer.
The robot currently resides in a hospital in Poland but scientists have shown the prototype at medical conferences around the world. And they have already been approached by doctors from Australia and Canada where it can take several hours to transfer rural patients to a doctor’s office or hospital.
“This is to support an initial diagnosis. The human is still in the loop, but this allows them to perform an examination remotely,” said Prof. Peer.

Telemedicine
The ReMeDi project could speed up a medical exam and save time for patients and clinics. Another EU-funded project – United4Health (U4H) – looks at a different technology that could be used to remotely diagnose or treat people.
“We need to transform how we deliver health and care,” said Professor George Crooks, director of the Scottish Centre for Telehealth & Telecare, UK, which provides services via telephone, web and digital television and coordinates U4H.
This approach is crucial as Europe faces an ageing population and a rise in long-term health conditions like diabetes and heart disease. Telemedicine empowers these types of patients to take steps to help themselves at home, while staying in touch with medical experts via technology. Previous studies showed those with heart failure can be successfully treated this way.
These patients were given equipment to monitor their vital signs and send data back to a hospital. A trial in the UK comparing this self-care group to the standard-care group showed a reduction in mortality, hospital admissions and bed days, says Prof. Crooks.
A similar result was shown in the demonstration sites of the U4H project which tested the telemedicine approach in 14 regions for patients with heart failure, diabetes and chronic obstructive pulmonary disease (COPD). For diabetic patients in Scotland, they kept in touch with the hospital using text messages. For COPD, some patients used video consultations.
Prof. Crooks stresses that it is not all about the electronics – what matters is the service wraparound that makes the technology acceptable and easy to use for patients and clinical teams.
“It can take two or three hours out of your day to go along to a 15 minute medical appointment and then to be told to keep taking your medication. What we do is, by using technology, patients monitor their own parameters, such as blood sugar in the case of diabetes, how they are feeling, diet and so on, and then they upload these results,” said Prof. Crooks.
“It doesn’t mean you never go to see a doctor, but whereas you might have gone seven or eight times a year, you may go just once or twice.”
Crucially, previous research has shown these patients fare better and the approach is safe.
“There can be an economic benefit, but really this is about saving capacity. It frees up healthcare professionals to see the more complex cases,” said Prof. Crooks.
It also empowers patients to take more responsibility for their health and results in fewer unplanned visits to the emergency room.
“Patient satisfaction rates were well over 90 %,” said Prof. Crooks.
Source: Phys.org



























Leave a Comment
You must be logged in to post a comment.